USA
USA 























If Not Imaging, Then What? The Science Points to Exercise
If structural abnormalities are nearly universal after 40, then the real question shifts: what actually drives shoulder pain and disability, and what effectively treats it?The answer, supported by a growing body of evidence, is exercise therapy, and specifically, targeted strengthening of the rotator cuff and scapular stabilisers. A systematic review and meta-analysis published in the Journal of Orthopaedic & Sports Physical Therapy evaluated exercise interventions that used the FITT principle (Frequency, Intensity, Type, Time) for rotator cuff–related shoulder pain. The evidence consistently shows that exercise reduces pain and disability, not because it fixes the structural findings on MRI, but because it restores functional strength, neuromuscular control, and joint stability.
However, exercise alone is not enough. The quality, specificity, and dosage of exercise matter enormously. As Hansford et al. (2022) highlighted in the British Journal of Sports Medicine: “If exercise is medicine, why don’t we know the dose?” Exercise interventions across health conditions are poorly standardised, limiting the ability to replicate successful outcomes at scale. This is precisely the gap that DAVID Health Solutions was built to close.
Introducing the DAVID Shoulder Solution: Where Precision Meets Practice
DAVID Health Solutions has developed what is recognised as the world’s only physiotherapy rehabilitation technology designed specifically for the treatment of shoulder pain, using medically certified exercise devices. The DAVID Shoulder Solution is not a general-purpose gym machine repurposed for rehabilitation; it is engineered from the ground up to meet the specific biomechanical demands of shoulder recovery.
The key insight behind the DAVID system is anatomical precision. Shoulder pain typically stems from weakness in the deep stabilising muscles, the internal and external rotators and scapular stabilisers rather than the larger, more superficial muscles. Conventional fitness equipment often misses these structures entirely, allowing dominant muscle groups, such as the pectoralis major, to compensate. DAVID devices are engineered to isolate the target muscles at optimal joint angles (including 60° abduction in the scapular plane for internal rotation work), preventing compensatory patterns and ensuring the right muscles are being loaded.
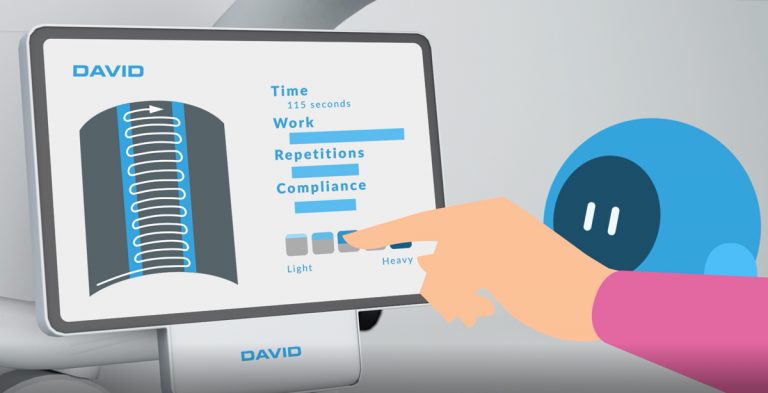
What sets DAVID apart from conventional physiotherapy tools, bands, pulleys, and free weights is the ability to quantify and control every parameter of exercise: range of motion, load, speed, sets, and reps are all defined numerically and tracked automatically. This solves the dosage problem identified in the research literature. Clinicians can now prescribe, deliver, monitor, and adapt shoulder exercise with the same precision we expect of pharmaceutical treatment.
The Devices: Built for Clinical-Grade Shoulder Rehabilitation
The DAVID Shoulder Solution includes a suite of devices, each addressing a specific movement pattern critical to shoulder health:
Glenohumeral Internal & External Rotation Devices
These devices provide pure, isolated rotation exercises for the shoulder joint. Biomechanically optimised joint angles enable safe and effective loading, even in acutely painful shoulders. The carefully engineered resistance curve follows the natural strength curve of the rotator cuff, loading lightly where the joint is vulnerable and progressively more where muscles are mechanically advantaged.
Diagonal Shoulder Abduction Device
This device features uniquely tilted movement arm axes designed to activate the scapular stabilizing muscles, a muscle group frequently neglected in conventional rehabilitation. The diagonal movement pattern is typically difficult to perform pain-free, but the DAVID system’s engineering makes it accessible even in the early stages of rehabilitation. All DAVID shoulder devices share core engineering principles: correct postural positioning, precise joint alignment, biomechanically appropriate resistance curves, and integrated biofeedback displays that guide patients through each repetition. Together, these features mean patients can train safely and independently after initial instruction, reducing therapist supervision time while maintaining treatment quality.
 Data-Driven Care: The EVE Software Platform
Data-Driven Care: The EVE Software Platform
The hardware is only one part of the DAVID ecosystem. The EVE software platform transforms exercise therapy from an art into a quantifiable science. Every training session is automatically captured, including range of motion, load, performance curve, adherence, and patient-reported pain scores. Clinicians access real-time dashboards showing objective progress. Treatment protocols are standardised yet individually adaptable, ensuring that what works can be replicated and scaled.This is exactly what the research calls for. When the JAMA Internal Medicine study questions the value of routine imaging, it implicitly calls for an alternative diagnostic and therapeutic framework grounded in function rather than anatomy. EVE provides that framework, replacing the “what does the MRI show?” question with “what can the patient do, and how are they improving over time?”
Who Benefits? The DAVID Shoulder Solution Across Patient Profiles
The DAVID Shoulder Solution is appropriate across a wide range of shoulder conditions and recovery stages, including prolonged or subacute shoulder pain, chronic rotator cuff–related conditions, post-operative rehabilitation following rotator cuff repair or shoulder arthroplasty, frozen shoulder (adhesive capsulitis), post-traumatic recovery, and recurrent or activity-related shoulder dysfunction.
Given that the new JAMA data shows rotator cuff abnormalities in nearly all adults over 40 — symptomatic or not — the DAVID approach is also highly relevant for prevention. Strengthening the rotator cuff and scapular musculature before pain becomes disabling is a sound strategy, particularly for ageing populations, office workers, and overhead athletes.Shoulder problems cause the most sick-leave days of any musculoskeletal illness (averaging 15 days per episode), are the most common musculoskeletal disorder in people over 65, and have tripled in prevalence over the past 40 years. Every second person will experience significant shoulder pain during their lifetime. The scale of the problem demands a scalable solution, and DAVID delivers exactly that.
The Takeaway for Clinicians: Less Imaging, More Exercise Science
The 2026 JAMA Internal Medicine study does not mean rotator cuff pathology is irrelevant, but it powerfully challenges the assumption that imaging findings should drive treatment decisions. When 96% of pain-free shoulders show rotator cuff abnormalities on MRI, those findings cannot reliably explain a patient’s pain, justify surgery, or predict recovery. What this study does support, alongside decades of exercise science, is a function-first, exercise-first approach to shoulder care. DAVID Health Solutions has built the clinical infrastructure to make this possible at scale: medically certified devices that isolate and strengthen the exact muscles that matter, paired with intelligent software that tracks every outcome.
The future of shoulder rehabilitation is not more scans. It’s better exercise, better measured. Scientific References1. Ibounig T, Järvinen TLN, Raatikainen S, et al. Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging. JAMA Intern Med. Published online February 16, 2026. doi:10.1001/jamainternmed.2025.79032. Hansford HJ, Wewege MA, Cashin AG, et al. If exercise is medicine, why don’t we know the dose? An overview of systematic reviews assessing reporting quality of exercise interventions in health and disease. Br J Sports Med. 2022;56(21):1238–1244.3. Efficacy of Exercise Therapy for Rotator Cuff–Related Shoulder Pain According to the FITT Principle: A Systematic Review With Meta-analyses. J Orthop Sports Phys Ther. 2024. doi:10.2519/jospt.2024.124534. Taylor A. Shoulder pain prevalence. J Rheumatol. 2005.5. Harkness EF, et al. New onset of shoulder pain: trends over 40 years. Rheumatology (Oxford). 2005.